
HuffPost reporters around the world are tracking the pandemic and the measures being taken to flatten the curve of transmission.
Read the latest updates on the coronavirus pandemic below. (To see the latest updates, you may need to refresh the page. All times are Eastern. For earlier updates on the pandemic, go here.)
All 50 States Have Now Begun To Reopen In Some Form — 5/20/20, 9:00 a.m. ET
Connecticut began to modestly ease some coronavirus restrictions on Wednesday, becoming the final state — out of the 42 that had issued stay-at-home orders — to start reopening in some form during the pandemic.
The Nutmeg state will now allow people to eat in outdoor sections of restaurants and visit retail shops. Offices, outdoor museums and zoos are also allowed to reopen.
Connecticut is taking “baby steps,” Gov. Ned Lamont (D) told CNN. “We have followed the metrics, hospitalization is down, fatalities are down. We have a lot of [personal protective equipment] right now. We have the gowns and masks. And finally, we have the contact tracing in place.”
Some governors who never issued statewide stay-at-home orders, like Iowa Gov. Kim Reynolds (R), loosened restrictions earlier this month on salons, tattoo parlors and other businesses.
— Hayley Miller
Brazil Records Grim New Milestone As Daily Death Toll Rockets — 5/20/20, 6:25 a.m. ET
The daily COVID-19 death toll in Brazil hit 1,179 on Tuesday, setting a new record for fatalities recorded in a single day by any country.
The figure is more than 250 more than the 919 deaths recorded by Italy in late March when it was the epicenter of the global coronavirus outbreak.
More than 18,000 people have now died in Brazil, according to official data, while 271,628 cases have been recorded, placing the country third behind the U.S. and Russia in total number of infections.
However, HuffPost Brazil reported that the true death toll is likely to be even higher due to the slow processing of laboratory tests.
On Tuesday, President Jair Bolsonaro doubled down on chloroquine as a possible remedy as Donald Trump said he is considering a travel ban from Brazil.
— Marcella Fernandes
Radicalized Instagram Stars Are Mainstreaming COVID-19 Conspiracy Theories — 5/20/20, 6:00 a.m. ET
HuffPost’s Jesselyn Cook reviewed Instagram accounts of more than a dozen seemingly radicalized influencers who have been using their platforms to push coronavirus misinformation. They try to discredit Dr. Anthony Fauci, claim that face masks are harmful, and push 5G conspiracy theories. With their large, dedicated followings, these women are in a unique position to open people’s minds to false and dangerous information.
— Liza Hearon
Indian Government Data Questioned As COVID-19 Cases Rocket — 5/20/20, 5:45 a.m. ET
The government of Prime Minister Narendra Modi is using incomplete data to justify its decisions and underplay the extent of the COVID-19 crisis, a HuffPost India report has found.
An analysis of publicly available data, local health bulletins, government documents, interviews with district and state-level officials, and infectious disease experts suggests that the highest levels of government do not have a real-time picture of how the pandemic is unfolding.
The government significantly relaxed India’s national lockdown on May 17, the day the country recorded the largest single-day spike in fresh coronavirus cases and fatalities.
India has recorded just over 100,000 cases and more than 3,000 deaths, according to official data.
Read more below:
NEW DELHI — On May 17, the day the Union government significantly relaxed India’s punitive national lockdown, the country recorded the largest single day spike in fresh cases of and fatalities due to the novel coronavirus.
The same day, Union Health Minister Harsh Vardhan said India had hit the 80,000 cases mark in 106 days after recording its first infection while many developed nations took just 44-66 days to reach that mark. The health ministry said the number of COVID-19 cases in the country were now doubling every 13.6 days, an improvement over the past fortnight, when cases were doubling every 11.5 days.
These cautiously upbeat statements and the easing of lockdown restrictions juxtaposed against the grim news of steadily spiking infections and fatalities reveal a worrying pattern: The Union government is using incomplete national-level data to justify arbitrary policy decisions, defend its record, and underplay the extent of the COVID-19 crisis.
HuffPost India’s analysis of publicly available data, local health bulletins, government documents, interviews with district and state-level officials, and infectious disease experts suggests that these imperfect numbers at best, offer an underestimate of the coronavirus’s spread, and at worse, form the basis for misleading conclusions to support arbitrary policy decisions.
Despite widely acknowledged inconsistencies and limitations of these data —the numbers are significantly dependent on India’s testing strategies and availability of testing infrastructure— senior health officials continue to display graphs at press conferences to give the illusion that the government is aware of how the pandemic is unfolding in real-time. Future projections of COVID-19 cases shared with states by the NITI Ayog and the Union Health Ministry are sometimes wildly divergent.
On April 11 for instance, the health ministry justified Prime Minister Narendra Modi’s controversial decision to lockdown the entire country without prior warning or planning, by presenting a graph that claimed India would have witnessed 800,000 cases by April 15 had the lockdown not been imposed. Experts questioned this projection, noting there was no explanation to justify these numbers.
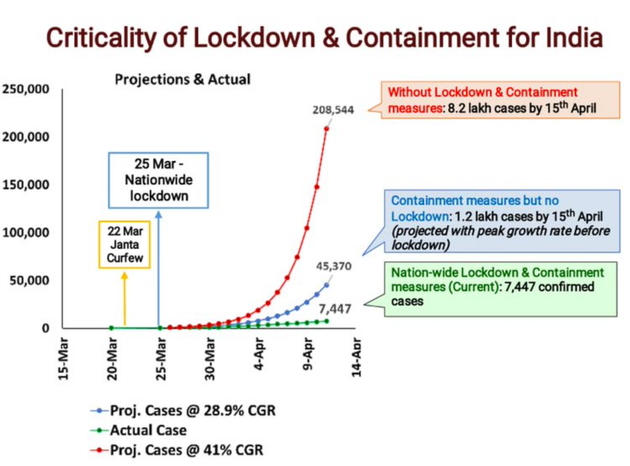
If the decision to impose the national lockdown on March 24 was justified on the basis of such ambiguous data and modeling, the government has offered no empirical explanation for the subsequent extension or easing for the lockdown.
To be sure, countries across the world have struggled to collate robust coronavirus statistics. But India, with its poor track record of data governance, has its own peculiar issues: Statistics routinely shared with the public by both the union government and state governments are compromised by long delays in processing tests, questionable interpretation of available numbers, and rudimentary modelling of India’s coronavirus crisis. This makes it hard to understand how the disease will spread over the next several days, weeks and months, when and where the number of cases will peak, and if India’s patchwork system of public and private healthcare will hold up.
The crisis in India’s data gathering, and the way this data is deployed by policymakers, is likely to become more pronounced in the coming weeks as travel restrictions ease and COVID-19 cases spike.
India’s narrow testing strategies and the limited testing infrastructure mean that even the highest levels of government do not have a real-time picture of how the pandemic is unfolding across the country.
The largely rosy view from the Union Health Ministry in New Delhi obscures vivid regional disparities across every metric used to measure the progress of the virus; making the case that states should have been given more freedom to devise their COVID-19 responses — including when and where to impose strict lockdowns — from the very beginning.
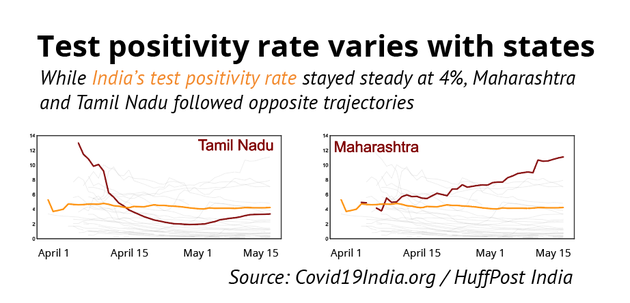
For instance, HuffPost India’s analysis suggests the country’s steady test positivity rate of 4% for several weeks (meaning there 4 positive cases out of every hundred tests conducted in India) appears to be a case of divergent regional trends cancelling each other out: On 10th April, Tamil Nadu’s test positivity rate was 10.8%, while Maharashtra’s was only 3.8%. By 16 May, Maharashtra’s positivity rate rose rapidly to 11%, while Tamil Nadu moved in the opposite direction to 3.4%. All this while, the national figures stayed flat at 4%.
Yet, the Union Health Ministry continues to speak in large, aggregate numbers that are essentially meaningless and devoid of context, and are occasionally used to present ludicrous scenarios.
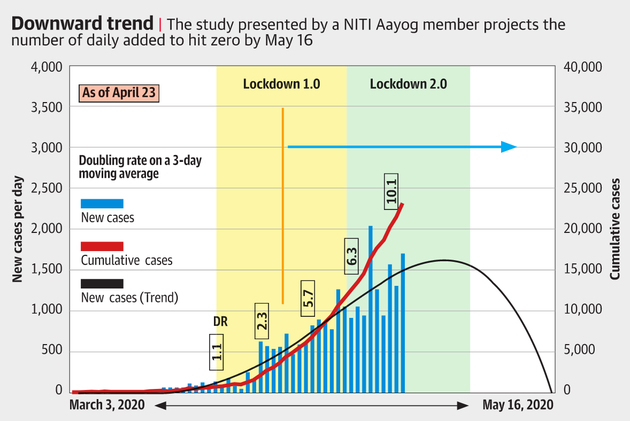
In a press conference on April 24 for instance, VK Paul, NITI Aayog and head of a government empowered committee on medical management, presented a slide suggesting that if current trends held, fresh cases were expected to trend to zero on May 16. In reality, as noted earlier, India reported the largest single day spike in coronavirus cases and fatalities on May 17.
“It makes a mockery of our response to the pandemic,” said Gautam Menon, a professor of physics and biology at Ashoka University, who researches infectious disease modelling. “What India and the world needs now is transparency and clarity regarding what is going on.”
“I recognise the desire of the government to present a positive face, but this should not be done by concealing data, by not revealing details of its preparation, by refusing to respond to genuine questions about its data and so on,” Menon said. Rather, Menon said, the government should maintain the trust of the public by being transparent in its presentation of facts.
Delayed tests
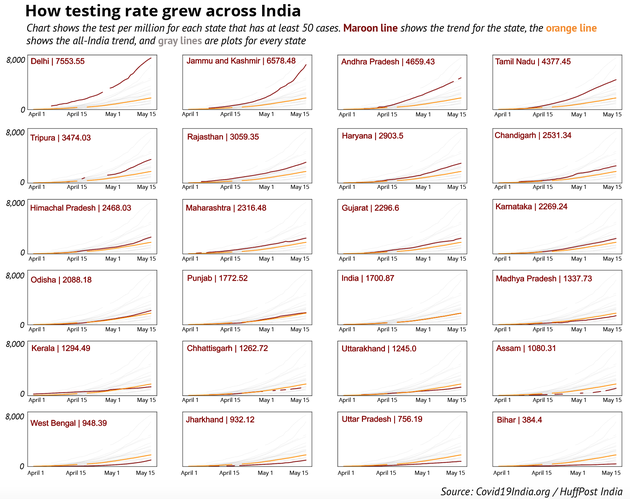
India’s testing trajectory is two-pronged. One one hand, the country has consistently ramped up testing, and now has a daily capacity to test over one lakh samples a day—only six countries have conducted more than India’s 2.4 million tests.
On the other hand, India’s vast population has meant the testing rate of 1,744 per million remains low. Of 149 countries to have reported at least 100 cases, only 33 have a lower testing rate than India, according to Worldometer.
As long as the testing remains limited, the number of confirmed COVID-19 cases will have limited meaning as well: increased testing might reveal more positive cases, but will not help us map the spread of the virus.
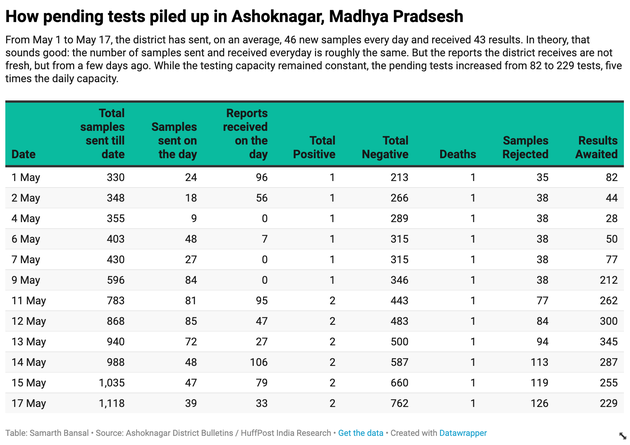
To understand how India’s attempts to contain the coronavirus have been hampered by the country’s persistent inability to test enough people and deliver timely results, consider Madhya Pradesh’s Ashok Nagar district, home to about a million people.
Ashok Nagar is a “green” district with only 2 COVID-19 cases thus far, but with train services resuming, the region expects thousands of workers stranded across the country to return home soon.
In the first day of May, Ashok Nagar had collected a total of 330 samples and received reports of 248 patients; the results of 82 samples were pending from April. By the 13th of May, the district had sent 940 samples, but a bottleneck in analysing these samples meant the number of pending samples had ballooned to 345 — more than four times the number of pending samples from a fortnight ago.
In a phone call, Ashok Nagar’s Chief Health and Medical Officer JR Trivediya confirmed the delays in receiving test results. Ashok Nagar’s experience can be extrapolated across Madhya Pradesh, say health activists.
“The backlog of pending samples awaiting results has been increasing at a rapid pace,” said Bhopal-based activist Amulya Nidhi of Jan Swasthya Abhiyan in a letter sent to the Union health secretary on May 6. “Patients were waiting for their test results and there are multiple instances of deaths happening before test results arrived.”
As of April 25, for instance, Madhya Pradesh had 9,021 pending samples against a daily testing capacity of around a thousand tests. This meant test results — on average — were delayed by nine days. The following day, Madhya Pradesh simply stopped publishing data on the number of pending tests.
In a fast-moving pandemic like COVID-19, this delay has significant real-world effects: For a health official in Madhya Pradesh hoping to use the data to figure hotspots, trace contacts, and prepare for an influx of patients, the state’s infection rate data would be obsolete well before it reached his desk.
Madhya Pradesh is not alone in hiding uncomfortable statistics. HuffPost India found only eight of the twenty large states publish pending tests data. On May 15, these states — Punjab, Haryana, Bihar, Chhattisgarh, Tamil Nadu, Kerala, Rajasthan, Uttar Pradesh — together tested around 36,000 samples on the day, and had a total backlog of 18,379 samples.
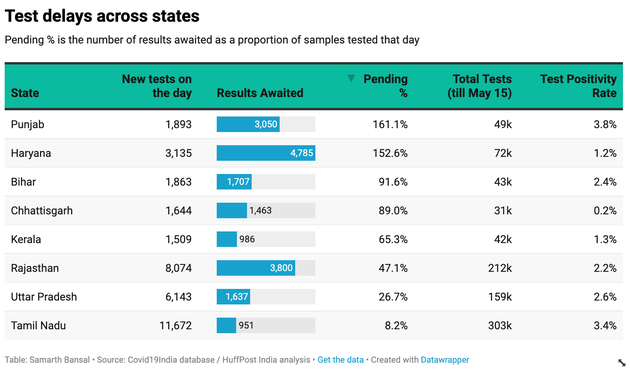
It is worth noting that the test positivity rate of all the eight states is less than the national average, meaning none of the states where the detected infection rate is higher have shared their data on test pendency. The available numbers do not tell us how widespread the delays are, a concern that anecdotal new reports from many states have raised where patients say they have waited for upto 10 days to receive their test results.
“Delayed test results lead to delay in getting individuals timely treatment and could lead to complications; it also affects contact tracing and breaking the chain of transmission,” said Genevie Fernandes, a public health researcher and postdoctoral research fellow at the University of Edinburgh.
“The first government response should be transparent reporting on websites and other forums regarding the delay in test results and also explaining the reasons for the same,” Fernandes said. “The second response should be fixing this delay.”
In this context, the record national spike of positive cases on May 17 doesn’t offer particularly helpful insights into the virus’s march across India — the “record” numbers simply indicate that the aggregated national level data across 36 states and union territories, each with varying degrees of delay and pendency, added up to the highest daily number till date.
Test positivity
The limitations of the numbers is just one concern. The manner in which they are interpreted in public is also contested.
Consider India’s low test positivity rate, which Union health officials use to reassure an anxious public that the coronavirus is not as widespread in India as it is elsewhere in the world and to deflect criticism that India, as a country, is not testing enough of its population.
At a press briefing on April 16, Dr Raman R Gangakhedkar, Head of Epidemiology and Communicable Diseases at the ICMR, referred to the low national positivity rate to justify the low rate of testing in India.
“In countries like Japan, one out of 11.7 tests turns out to be positive, which is among the highest in the world. Italy tests 6.7 persons for one positive test while the USA tests 5.3 persons and the United Kingdom 3.4,” Gangakhedkar said at the press conference.
“Taking their population base into consideration, it is difficult to comment about our testing rate,” Gangakhedkar said. “In India, we are conducting 24 tests out of which one comes out to be positive. Also, we have a huge population and not all people belong to vulnerable groups. Hence, can’t say our testing ratio is low.”
But experts say that India’s test positivity rate is more reflective of the country’s testing strategy.
“Our testing criteria is limited. We are not conducting widespread testing regardless of symptoms, hence we will not know the true figure of those who have the infection in a population,” Fernandes, the public health researcher, said. “Hence, the assumption of reduced transmission owing to the low test positivity rate at the national level may not hold true.”
A deep dive into state-wise test positivity rates shows the number fluctuates significantly. As mentioned earlier, in states like Maharashtra, the test positivity rate has risen significantly as the government expanded testing, while Tamil Nadu has witnessed the opposite trend.
Perhaps the most vivid example of the unpredictability of test positivity trends, and a good reason to test as widely as possible, is the case of Bhilwara in Rajasthan which gathered national attention as one of the first hotspots, and was subjected to what was described as a ”ruthless lockdown”.
Today, the district with 2.8 million population has done 15,993 tests—5,711 tests per million, more than three times the national average— with a test positivity rate of just 0.5%, ten times lower than the national figure.
“The national figure definitely makes no sense in the context of a disease which is spreading very differently in different parts of the country,” Menon of Ashoka University said, referring to the wide variation in the test positivity rates.
Modelling woes
At a press conference on April 24, VK Paul, NITI Aayog and head of a government empowered committee on medical management, displayed a surprising slide suggesting the number of new cases would go to zero on May 16, which, according to The Hindu, members of Paul’s own committee didn’t agree with. May 16, coincidently, was a day before Prime Minister Modi’s second extension of the lockdown was scheduled to end.
Paul subsequently walked back his remarks in a statement to Caravan, suggesting “that was a trend line” without offering any further details, but the slide is a worrying illustration of the quality of the modelling and future projection scenarios panning out in India that are central to managing the pandemic response.
“Those were ridiculous predictions, especially because the methodology that led to them has never been disclosed,” Menon said. “So it is impossible to say whether there is a real epidemiological model behind them or not. Anyone can plot a function that runs through a given set of points.”
The government’s own internal projections, shared amongst officials but not with the press, suggest that the public claims are carefully choreographed to manage the national narrative.
Take Punjab. According to the task force report on the existing lockdown strategy released on April 25, the state was presented with three different projections: from the Punjab’s health department, NITI Aayog and the Union health ministry.
The health ministry projections for Punjab said the state would need 602 ICU beds by 24 May while NITI’s estimate was six times, at 3612 beds. In fact, NITI— of which Paul is a member—told the state to expect 3,680 new cases per day from 31 May.
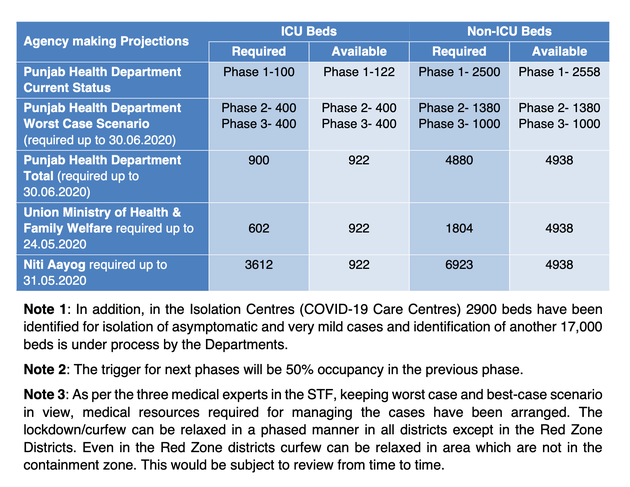
An official who helped the state task force said Punjab had not been provided details on how these projections were arrived at, which meant they could not reconcile why the numbers from the Centre were significantly higher than the state’s own health department.
“Data science should be transparent. All models are wrinkled with assumptions but it should be clear what the assumptions are,” said Bhramar Mukherjee, a professor and chair of biostatistics at the University of Michigan.
The opacity of much of India’s modelling does not allow external experts to evaluate the built-in assumptions—a critical component of improving the models. Neither is the public informed of the basis on which decisions are being made.
Models, Mukherjee said, should not be quoted or taken as destiny for their exact numbers as there are huge uncertainties associated with the projections, but to help decision makers evaluate likely scenarios based on possible interventions.
Thus far, details of only one modelling project, MedInventory—which was facilitated by Principal Scientific Advisor to the Prime Minister—are in the public domain. It provides district-wise projections for the healthcare infrastructure requirement in the next four weeks. However, it is not clear who is using it.
Health officials of three states—Telangana, Andhra Pradesh and Tamil Nadu— told HuffPost India they were not using the MedInventory website. Instead, agencies at different levels of government are making their own projections.
“Even though the state had also requested the Ministry of Health for projections in April, Andhra Pradesh has been relying on its own projections arrived at by expert committees which have access to data compiled by the state,” a state health official of Andhra Pradesh explained. “Based on the state’s projections, AP has readied a total of 50,000 beds for Covid-19 patients for June-July.”
Doubling rate obsession
Across the country, most health officials continue to speak in terms of “doubling rates”, the time taken for the number of COVID-19 cases to double in number, to make future projections.
“We are keeping track of the doubling rate,” said Pradip Awate, state surveillance officer of Maharashtra. “ As of May 13, it stands at 10.2 days. So if we have 24,000 cases today, we are projecting 48,000 cases after 10 days, and accordingly we think of the capacity needed.”
Awate said the state does not make district-wise projections.
But experts raise questions about this metric.
“The doubling time is a crude measure. It is a measure on the relative scale,” Mukherjee from the University of Michigan said.
“For prioritization and resource allocation you need an idea about total case-counts, hospitalization counts and estimated counts for those that will seek critical care. I am not sure how ‘doubling time’ will help with these projections,” she said.
“I wish there were more savvy statisticians working closely with the government,” Mukherjee said.
Menon, the Ashoka University professor, said that the doubling rate is not a bad proxy in the early part of the epidemic when the disease is in its exponential growth phase to tell what might happen in the next few days. “But once the case numbers begin to drop, this approach will of course make no sense at all,” he explained.
“The doubling rate ignores the fact that the disease spreads at different rates in different places,” Menon said. “It will spread slowly in places where physical distancing is taken seriously, mask wearing is common and hand-washing and similar measures are prevalent. It will spread fast in dense crowded regions where none of these is attended to.”
“So to use a single doubling rate across a whole state can mask the growing number of cases in districts and sub-districts, since it is a less granular measure,” Menon said.
Over a long period of 6 to 8 months, Awate, the Maharashtra official said, the state is expecting 0.5% of its residents to be infected with the virus, of which 15% would need hospital treatment and 5% would need critical care—and the state is ramping up its healthcare capacity accordingly.
“We are hoping for the best and preparing for the worst,” Awate said.
— With inputs from Nikhila Henry in Telangana
Credit: Source link