One of the indescribable aspects of being a member of a minority group is knowing that things are better than they have ever been and, simultaneously, not good enough.
The LGBTQ community has won the right to same-sex marriage and achieved unprecedented visibility in politics, media and entertainment. Yet we still lag far behind the straight and cis population when it comes to mental health, substance abuse and HIV rates.
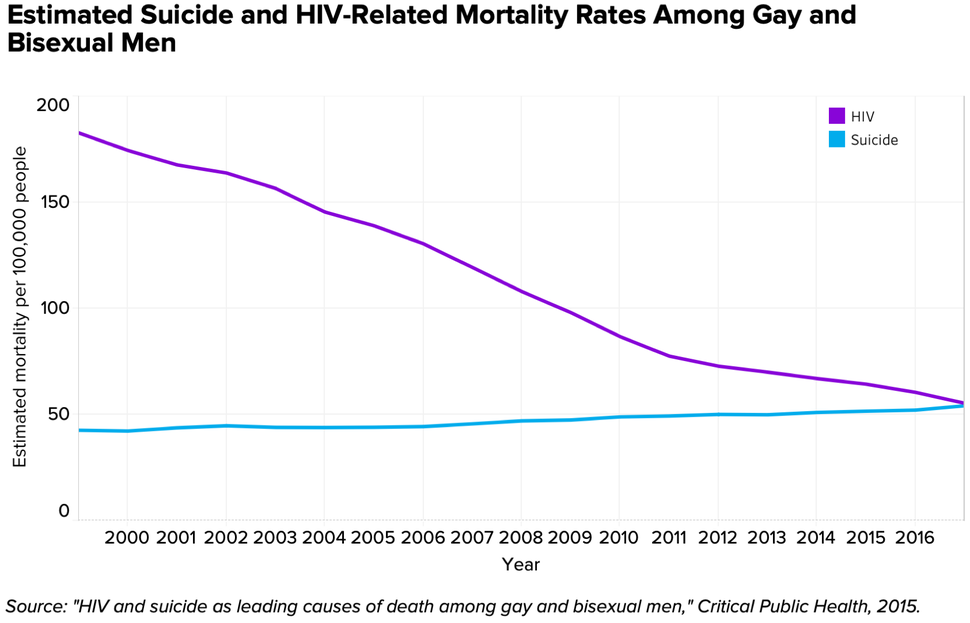
Travis Salway is an epidemiologist trying to close this gap. In 2014, he discovered that in Canada, suicide had surpassed HIV as the leading cause of death among gay and bisexual men. More recently, he’s been advocating to outlaw conversion therapy and offer mental health screenings at clinics that diagnose and treat sexually transmitted diseases.
HuffPost talked to Salway about these persistent challenges and the fight for health equity.
How did you find out that more gay and bisexual men were dying of suicide than of causes related to HIV?
I had been working in HIV prevention for years, motivated by the fact that new HIV infections weren’t coming down among gay men. One of the theories we were exploring was that social isolation, depression, drug addiction and other social factors were leading to sexual behavior associated with HIV transmission. These same factors, of course, can also lead someone to suicide.
I pulled the suicide statistics among gay and bisexual men and was really shocked at how high they were. Though HIV mortality rates had been declining for years, suicide rates remained stable. When we ran the numbers, we found that around 2007 the lines crossed and suicide surpassed HIV as the leading cause of death. Since then they’ve continued to diverge, and by now the difference between them might be twofold.
Why do suicide rates remain so high among the LGBTQ population?
The predominant theory is called “minority stress.” The idea is that sexual minorities accumulate stressors in multiple forms. That includes overt things like beatings and name-calling, but also quieter things like avoiding a family gathering because you don’t want to have an awkward conversation with your uncle. Even if no one ever says it, you get the message that you’re wrong.
Minority stress continues even after you’ve left the closet. All of us, all the time, have to decide when to come out. Even if you’re in a big city, Castro-style environment where everyone is all “yay gay,” there’s still cognitive stress every time you make that decision.
Over time, minority stress leads to problems like rumination — thinking negative thoughts over and over again. It can lead to a sense of hopelessness. Some people cope by self-medicating with drugs or alcohol. Some withdraw in social situations and use substances to connect.
And we’re now learning that sexual minorities have structural risks that go beyond spending their adolescence in the closet. Marriage, children, access to jobs and support networks are all different for sexual minorities in ways that are relevant for suicide. People who have steady partners, for example, are generally less likely to kill themselves. Gay and bisexual men are less likely to be in long-term relationships and tend to start dating much later in life. That may be another risk factor in suicide.

It seems like an important conclusion from your work is that the “It gets better” narrative is much more complicated than the slogan suggests. It’s not a straight line of progress, it’s this cluster of overlapping challenges, some of which are getting better and some of which are getting worse.
Exactly. There’s this new research showing that queer adolescents are coming out earlier. That sounds great, right? But they’re not actually doing all that much better in schools. They’re still feeling isolated. There are these initiatives in schools, like gay-straight alliances now. For the kids who can benefit from them, that’s great. But a lot of kids have too much internalized homophobia, or are too afraid of bullying, to ever participate in a group like that. So many of my interview subjects who attempted suicide have told me they’ve walked right up to the door of support groups and turned around. Those are the people at the highest risk of suicide, and they’re the hardest to reach with the service model we have now.
One of your current projects is advocating for the inclusion of mental health care in STD clinics. Why is it important to deal with the crisis that way?
One of the great achievements of the gay community in the last four decades is the creation of this incredibly sophisticated infrastructure for testing and treating and preventing HIV. We don’t have anything like that for mental health and suicide. We need to adapt that infrastructure to the crisis we face now. STD clinics are places where we can catch people before they fall through the cracks.
Because of minority stress, we know that queer people will delay or avoid mental health care if it’s not available to them. They might go to the doctor’s office for a sprained ankle, but they won’t say anything about their depression or drug use for fear of being found out. And that’s assuming they’re going to the doctor regularly and that they have a doctor to go to at all, neither of which is a given.
The reason STD clinics work so much better for mental health is that they’re low-barrier. You don’t show your ID, you don’t give your name and they’re free even if you’re coming from out of the state or out of the country. This means patients are much more likely to reveal their mental health concerns than at other clinics, or even to their family or friends.

Where should the LGBTQ community focus resources when it comes to public health?
The next wave of gay rights needs to be about building meaningful, lasting social supports that withstand the three major threats we face.
The first threat is the loss of the “gayborhood.” Many of the traditional gathering spots have already moved online. But, more importantly, the cities with the greatest concentrations of gay people are becoming unaffordable. Young gay people are being forced to move way out into the suburbs or to smaller cities where there’s fewer services. We need to learn how to reach those populations.
The second threat is aging. Forming a family is one of the most powerful protections against suicide for straight people. Queer people are less able to do that. Loneliness and social isolation are huge problems in our community, and they seem to get worse as we age.
The third threat is stratification within our own population. What does it mean to offer services to a community that contains hedge fund managers and homeless teenagers? The disparities in needs within the LGBTQ community are profound, and we need specific supports for the groups at the highest risk.
What brings us together is this feeling of finding a way forward in a world where you’ve always known your life was going to be different. Partly due to the legacy of the HIV epidemic, we’ve designed a lot of our spaces around the needs of gay men. But where do our queer women go when they are facing a mental health crisis? We need to look at a much broader range of needs and offer brick-and-mortar spaces to form community.
I don’t want to say this isn’t happening already, but we need to rally around the health of our community the same way we rallied around same-sex marriage. That was a good effort, but it’s time to dig deeper.
If you or someone you know needs help, call 1-800-273-8255 for the National Suicide Prevention Lifeline. You can also text HOME to 741-741 for free, 24-hour support from the Crisis Text Line. Outside of the U.S., please visit the International Association for Suicide Prevention for a database of resources.
REAL LIFE. REAL NEWS. REAL VOICES.
Help us tell more of the stories that matter from voices that too often remain unheard.
Credit: Source link