Above: Jonathan White with his family. Illustration: HuffPost; Photos: Family Handout/Getty Images
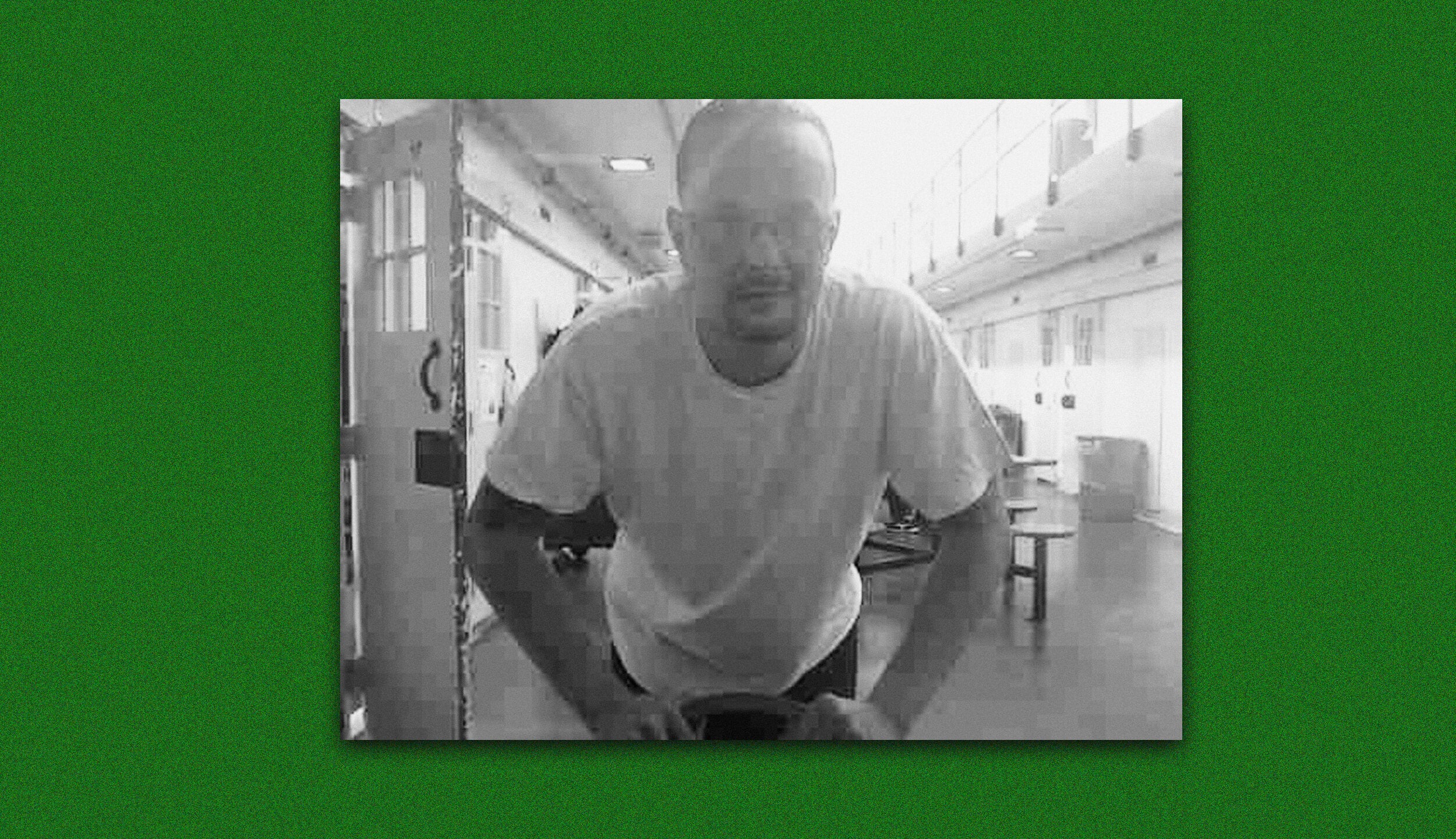
Jonathan White, a 45-year-old man incarcerated at a state prison in Ohio, gazed out at the group of people who had come to collect their lunch from the chow hall. As part of the effort to contain the spread of COVID-19, people were sent one dorm at a time to pick up their food. These individuals were from the dorm that houses many of the people who are elderly or have health conditions.
“My heart just ached cause I asked myself who am I seeing now that I won’t see again due to death from this virus,” White wrote in early April, just as the pandemic was building toward its first peak in the U.S.
“This prison is just too crowded, there is no way everyone will make it that I’m seeing unscathed,” White wrote. “Thanks to years of flopping people simply because they have the power to, never truly looking into who people are today,” he continued, referring to those he knew who had been denied parole. “This has resulted in their apparent overall objective which is to see to it that as many people as possible die in prison.”
Since White made that dire prediction, at least 13 people incarcerated at Marion Correctional Institution (MCI) have died, in addition to at least one prison staff member. More than 2,000 prisoners — about 80% of the population — have tested positive for the coronavirus, including White. The prison is the second-largest COVID-19 cluster in the country, according to the New York Times tracker, just ahead of Pickaway Correctional Institution, another Ohio state prison about an hour away. Nationwide, 9 of the top 10 coronavirus clusters are in prisons or jails.
There are signs this particular prison outbreak spread into the surrounding community: The relatively small county of Marion has one of the highest rates of infection in the state, even with the Marion prisoner cases removed from the count.
HuffPost spoke with eight people incarcerated at Marion for more than two months about what it was like living through the pandemic, knowing it was almost impossible to avoid the potentially fatal disease behind bars. They described how their prison sentence stripped them of the ability to make decisions that would increase their chances of survival. They did everything within their power to protect themselves from COVID-19: They followed the news closely. They requested masks but were denied until it was too late. They pleaded with prison staff. They filed internal complaints, knowing they would go nowhere. They filed lawsuits, sometimes without help from a lawyer or access to the internet.
And when they turned on the TV, they watched the governor and the head of the state’s Department of Rehabilitation and Correction — officials with immense control over their fate — mislead the public about the protections available to people in the state’s prisons.
The coronavirus outbreak at the prison in Marion is proof of what criminal justice reform advocates and incarcerated people have been warning since the beginning of the pandemic: It is nearly impossible to keep the coronavirus out of prisons and jails, and once it’s in, it endangers everyone who lives and works in and around the facility. It is a risk that disproportionately impacts Black people, who are more likely to be incarcerated and also more likely to die of COVID-19. In April, the prison at Marion was dubbed the “number-one coronavirus hotspot” in the country — but because of a lack of mass testing in most American prisons, it’s impossible to know if Marion is truly an anomaly or if it’s indicative of how the highly contagious disease is traveling through similar detention facilities.

As the scale of the epidemic revealed itself in March, many Americans began frantically preparing: stockpiling groceries and cleaning supplies; making improvised masks and learning to avoid getting too close to strangers. Every interaction was freighted with intentionality, as people made careful judgments about who was safe and who was a possible risk.
Inside Marion, however, a shambolic and ultimately futile version of this pandemic preparedness was taking place. Prison officials tried to replicate some of the medical guidance. They sent frequent messages through JPay, a corrections messaging service, urging people to wash their hands and practice social distancing. But even the simplest suggestions seemed absurd.
A grim alternate reality took shape. People incarcerated at Marion knew some of them would die from the coronavirus. They closely followed media reports about the emerging pandemic, and what was happening inside the prison did not match the urgent warnings they saw on TV in early March.
“There are three feet in between my bunk bed and the bunk bed on my left side and the bunk bed on my right side,” Steven D’Augustino, a 50-year-old man with asthma who is incarcerated at MCI and has tested positive for COVID-19, said in a May interview. “So I have a living quarters, if you don’t count the bed itself, of about 18 to 21 square feet — two people actually, myself and my bunkie have about 21 square feet.”
When people pointed out the physical impossibility of social distancing, given their living conditions in a prison operating at more than 150% capacity, they were instructed to sleep “head-to-toe,” D’Augustino said.
The prison started conducting temperature checks on employees coming to work on March 11 — but in the early days of the pandemic, the virus was being spread by people who did not yet run a fever or exhibit other symptoms.
Like other front-line workers, prison employees who wanted to wear masks had a hard time getting them. “We do not have the masks to issue to every staff member,” a corrections department official wrote in an email obtained by HuffPost, referencing the shortage of N95 masks. After weeks of unsuccessful negotiations, the Ohio Civil Service Employees Association — the union that represents the state’s corrections officers — used $200,000 in member dues to buy its own supply of KN95 masks to distribute to workers.
On March 25, the first corrections officer reported feeling sick. The officer had worked in the prison the previous day. It became clear the temperature-check firewall for employees had failed when the officer tested positive for the virus on March 29 — and when others began testing positive in the following days.
Several corrections officers who tested positive returned to work before they had recovered. Public health officials have urged Americans who contract the coronavirus to stay home until they’ve gone three days without a fever, have no respiratory-related symptoms, and have gone 10 days since symptoms first appeared. But that timeline wasn’t realistic for Ohio corrections officers, who received only 40 hours of paid leave for COVID-19.
Even if every officer was meticulous about stopping the spread of the virus, they were in an almost impossible situation. But some corrections officers didn’t seem to take the threat seriously, several people incarcerated at MCI said in interviews. Prisoners overheard guards inaccurately claim that the coronavirus was less deadly than the flu, a common talking point in right-wing media and one often repeated by President Donald Trump in the early weeks of the pandemic. Several prisoners who tried to cover their faces with makeshift masks were told to remove the coverings or risk getting written up for “contraband,” two incarcerated individuals said in interviews.
JoEllen Smith, a spokeswoman for the Department of Rehabilitation and Correction, confirmed to HuffPost that “wearing masks would have been a serious violation” of prison rules “prior to COVID.” The DRC did not adjust the guidance to allow masks until March 27 — and did not require them until April 7. Even then, incarcerated individuals were initially given only one mask, meaning they would have to go barefaced while they were washing it by hand and letting it dry.
So some 2,500 people sat inside the overcrowded prison, waiting for the virus to reach them. There was no hope that Ohio officials would thin out the prison population, which would have allowed freed individuals to protect themselves and created more space for those who remained behind bars. Although Ohio Gov. Mike DeWine was one of the few Republican governors willing to break with Trump and acknowledge the severity of the situation in the early days of the pandemic, he refused to meaningfully reduce the state’s prison population.
Asked during a March 29 press conference if he was considering letting anyone out of jail or prison, DeWine suggested that those incarcerated were safer in crowded detention facilities than out on their own. “What makes us think that they’re going to be in any better position outside than inside?” said DeWine.
A person incarcerated at Marion tested positive later that week.

The prison, which had already suspended visits from family and lawyers, went into lockdown. The things that make prison more bearable — educational classes, access to the library — were shut down indefinitely. Confined to their living areas for nearly the entire day, people had almost nothing to distract them.
“That’s OK if they’re really protecting us. The problem is they obviously didn’t protect us,” D’Augustino said.
The first COVID-19 death directly tied to the prison came on April 8. John Dawson, a 55-year-old corrections officer, had worked in the control center giving out equipment to prison staff. He had been with the Department of Rehabilitation and Correction for 24 years.
Keeping the virus out of the prison appeared to be a lost cause. Dennis Salerno, a 50-year-old man incarcerated at Marion who describes himself as a “health nut,” often prepared a drink that includes cayenne pepper for himself and a friend. He realized they were sick when neither of them could taste the cayenne. “Cayenne is hot!” he said in an interview. After adding a third of a jar of the pepper, Salerno decided he should stop adding more — “and that certainly we had Corona.”
Officials’ focus shifted to mitigating the damage. Meals were reduced to twice a day to limit movement within the prison and allow time to clean the cafeteria between groups coming to pick up their food.
People inside had little confidence these measures were sufficient. White, who has high blood pressure and hypertension, started worrying that his job in the chow hall’s recycling unit was putting him at an even higher risk of getting the virus. But if he refused to show up, he risked punishment and a disciplinary report that could jeopardize his chances of being granted parole in the future.

After talking with his family, White decided to stay in his dorm and do his best to self-quarantine. When he didn’t show up for work, corrections officers threatened to extract him from his cell and place him in solitary confinement, he said. He eventually received permission to pause his work at the chow hall after his family intervened. (Smith, the DRC spokeswoman, told HuffPost that the department had “nothing on record to verify this occurred” but did not deny White’s account.)
White’s precautions weren’t enough. He lost his sense of taste first — and then his ability to catch his breath. “My breathing had gotten so bad I had to turn my TV off and just focus and breathe. It was like trying to catch a feather,” he said. He self-treated the problem by holding his head over a crockpot and inhaling the steam. “It helps your skin,” he joked.
D’Augustino soon found himself literally surrounded by people who were sick. “Two people to my right had lost their sense of taste, the person that sleeps on the bottom bunk to my left was coughing, I was coughing, people around me were coughing ― I mean there was just all kinds of symptoms all over the place,” D’Augustino said.
“Guys was just falling out left and right,” said Shannon Kidd, a 42-year-old man imprisoned at Marion. The prison staff “was so overwhelmed with it, I don’t think they had the right staffing in place to handle it,” he said.
Members of the Ohio National Guard were dispatched to the prison as more staff members called in sick. Prisoners with high fevers were removed from the dorms. The people they lived with never found out where the sick were taken — although they feared it was to solitary confinement.
Solitary confinement is a form of torture and nobody inside wanted to end up there. Smith told HuffPost that people who are quarantined due to illness in areas typically used for punishment are not subject to the rules typically associated with solitary confinement — but those incarcerated at Marion didn’t know that. The fear of solitary drove some people to drink ice water and put cold towels on their heads before temperature checks in hopes of masking a fever.
Then, prisoners started to die. Jesse Zeigler, 74, told his family on April 6 that he was having trouble breathing, body aches and a headache. Christine Bevington, Zeigler’s stepdaughter, said a nurse at the prison told Zeigler that he didn’t have a high fever but that he should let her know if his symptoms worsened. Bevington worried that her stepfather was struggling to speak over the phone and called the prison’s medical staff. She found out days later that he was admitted to the hospital and diagnosed with COVID-19.
While Zeigler was in the hospital, Ohio’s corrections department began mass testing every person at three of the state’s facilities with the largest COVID-19 outbreaks, including Marion. “It seemed like it was a little too late,” said Andre Stores, a 43-year-old man at Marion with hypertension and pre-diabetes who tested positive for the virus. “Everyone was sick at the time.
When the results came back a few days later, some of the people imprisoned at Marion learned about the severity of the outbreak on the news: 78% of the prison population tested positive in that first round. In less than three weeks, MCI went from one confirmed COVID-19 case on staff to 154 staffers and 2,011 incarcerated people infected with the virus.
Meanwhile, Zeigler’s health was deteriorating — but his family remained largely in the dark. His wife received a call from someone offering information about a support group. “She told them she didn’t need it,” Bevington said in an email. “She didn’t know her husband was dying.”
On April 19, Zeigler’s wife received another call, telling her that he had been on dialysis and a ventilator and probably wouldn’t make it through the night. The hospital arranged a Zoom video call for the family to say goodbye. He “was not responsive but we talked to him and told him we love him,” Bevington recalled. Before hanging up, Bevington asked the nurse if someone would call to let the family know when Zeigler passed away, and the nurse agreed.
Zeigler’s wife found out he was dead the next morning around 10:45 when she received a call from Ohio State University’s Wexner Medical Center asking if she wanted an autopsy. He had died the night before, she learned, less than an hour after the Zoom call ended.

Marion Correctional Institution had become the nation’s worst documented COVID-19 hot spot. (It has since been replaced by Los Angeles County’s jail system.) The New York Times editorial board referenced its surging case numbers in a piece urging states to free prisoners to prevent more people from dying in custody. MSNBC broadcast videos sent from people incarcerated at Marion describing unsanitary conditions inside the prison.
But is Marion’s outbreak actually exceptional? Very few correctional institutions do facility-wide testing, as was undertaken there in April, and so there is little information about how many people have contracted the virus in other prisons and jails. This lack of data leaves open the alarming possibility that other prisons have infection rates similar to — or worse than — Marion’s.
In places that are doing limited or no COVID-19 testing, “their case rates look really low — but it’s really artificial because if you don’t have testing in the door, there’s no way to know what true prevalence is,” said Lauren Brinkley-Rubinstein, a co-founder of the COVID Prison Project, a group of public health scientists who track the coronavirus in correctional facilities.
Several states with high rates of testing — including Michigan, Tennessee and New Jersey — uncovered high rates of infection, researchers at the COVID Prison Project have found. Although no other prison has reported numbers as stunning as those at Marion, mass testing consistently shows that COVID-19 cases are more widespread behind bars than previously acknowledged.
The vast majority of prisons only test very visibly ill individuals and are almost certainly undercounting people who don’t show symptoms or who don’t report symptoms out of fear of being sent into solitary confinement. In Ohio, the corrections department had initially planned to do mass testing in every prison where limited testing revealed positive cases, Christopher Mabe, president of the corrections officers union, said in an interview in May. But after mass testing at Marion revealed catastrophic rates of infection, the corrections department shifted to supposedly more targeted strategic testing.
“They have walked away from the testing, basically burying their head in the sand on the actual problem that still exists,” Mabe said.
Corrections departments have incentives to avoid mass testing. It’s expensive, there are logistical complications to administering the tests, and the results could reflect poorly on the department. Most corrections departments are either unable or unwilling to acquire enough materials to commit to ongoing testing.
And because corrections authorities and politicians have mostly refused to significantly depopulate prisons, there isn’t room in most facilities to segregate COVID-19 carriers from everyone else. So without a plan in place to meaningfully protect incarcerated people from the coronavirus, mass testing does little more than document the system’s failures.
With mass testing, “the risk is that you find a lot of people and it makes you look bad,” Brinkley-Rubinstein said.
Other states are selectively testing prisons, too. At Washington state’s Monroe Correctional Complex, one of the first prisons nationwide to confirm a COVID-19 case, conditions are similar to those at Marion: Prisoners live in crowded dormitories as opposed to single cells. Washington and Ohio’s corrections departments have both responded to the pandemic by suspending visitation and programming, isolating symptomatic prisoners, implementing temperature checks for staff, restricting movement within the prison, and encouraging social distancing. But Washington has not conducted mass testing at Monroe — and claims that only 20 people incarcerated there have tested positive for COVID-19.
On June 17, the Washington State Department of Corrections announced plans for widespread testing at a different prison, Coyote Ridge Corrections Center, after confirming more than 100 COVID-19 cases among prison staff and incarcerated people. The state tested those people incarcerated in the medium-security complex and employees throughout the prison, and the number of confirmed cases more than doubled. The corrections department did not respond to an email asking why they were not conducting mass testing in every prison with confirmed cases of the coronavirus.
The corrections department is moving some of the people who tested negative out of Coyote Ridge, but the effort comes too late to save some lives. Victor Bueno, a 63-year-old man incarcerated there, died from COVID-19 the day after the testing plan was announced. Bueno was set to be released in three months. A second man, 72-year-old William Bryant, died four days later.
Some of those incarcerated at MCI didn’t learn their own diagnosis until after seeing on the news that most people in the prison had tested positive for COVID-19. They received their results on a stapled-shut piece of paper. For some, it was almost a relief to receive confirmation of a diagnosis they had already suspected.
The test results triggered a haphazard effort by prison officials to separate the people who tested positive from the people who tested negative. It did not go well.
“They have no clue how to separate,” said Geoffrey Banks, 37, who is incarcerated at Marion and tested positive for the coronavirus. “At first, it was we’re going to separate all the positives. We’re going to make the gym and these couple dorms all positive,” Banks said. “Then they realized, ‘Wow, you know, there’s a lot more positives than we thought.’”
So the gymnasium and other areas used to quarantine the COVID-19-positive group flipped to become the areas to hold the people who tested negative. Smith, the DRC spokeswoman, said that if the positive and negative groups switched places, those areas would have been “thoroughly cleaned and disinfected,” but people inside don’t think it was enough. “They cross-contaminated that — they just screwed the pooch on that one, for lack of a better term,” Banks said.
By moving people with COVID-19 symptoms around in an attempt to create isolation areas, MCI staffers may have “inadvertently spread it a little bit,” Traci Kinsler, Marion County’s public health commissioner, said in an interview.
Even after it became clear that most of the prison was infected with COVID-19, people who were sick had a hard time getting medical attention. “The only way medical was taking guys was guys that were falling out,” White said
Banks, who experienced severe stomach pains, chills, headaches, fatigue and a slight fever, said that “unless you are not breathing, they’re just gonna give you Tylenol or stomach pills and send you on your way.” Some of Banks’ symptoms continued through late May, more than a month after he tested positive for COVID-19. “I am having labored breathing and can’t lay on my back without feeling like I have a bowling ball on my chest as well as a heavy cough,” he told HuffPost in a May 15 message on JPay. He waited several days for a response to a health services request and eventually received a cough expectorant, which he worried would just make him cough more. (Smith contends that people held at Marion had “adequate access to medical care” and could request emergency help.)
Testing doesn’t always deliver clear results, and some prisoners at Marion received inconclusive results and had to get retested the following week. In the meantime, they were left in the same living area as the people who tested positive.
Willis Williams, a 64-year-old with a liver disorder and hypertension, was one of the people who had to get retested. His second test results came back negative at the end of April, but he was never moved away from the COVID-19-positive population. Prison staffers told him the people who tested positive had probably recovered. Williams thought that was unlikely. And even if it was true, some of the people he got retested with received positive results the second time around, including individuals who lived in his dorm, he said.
“They left me in a positive area knowing that I was negative. They started off trying to separate positive from negative and then they take forever to get my results and then when I do test negative, they say, ‘Oh well, stay where you’re at,’” Williams said in an interview. “That’s kind of difficult to swallow. There’s not a lot I can do.”
Asked if he ever suspected he’d caught the coronavirus from someone in his dorm, Williams said it was hard to tell. “When you’re worried, your mind plays tricks on you. You cough too many times and wonder if you have it,” he said. “It was kind of traumatic to go through this every day not knowing.”
Ohio’s corrections department has attempted to downplay the severity of the situation by emphasizing that many of the people who tested positive were asymptomatic individuals who wouldn’t have received a COVID-19 test at most other prisons. Annette Chambers-Smith, the department’s director, claimed in a May 18 press conference that 96% of the incarcerated people who tested positive were asymptomatic. Several individuals held at Marion told HuffPost they believed they were incorrectly classified as asymptomatic if they didn’t have a fever or shortness of breath, even if they reported other symptoms.
Chambers-Smith eventually acknowledged that more than 4% of the incarcerated people who tested positive experienced symptoms of the disease. “As the [Centers for Disease Control and Prevention] recognized additional symptoms of COVID, those things were added to our verbal screening process,” Smith, the DRC spokeswoman, wrote in an email.
Undercounting the number of symptomatic people could be a way to deflect criticism over the department’s handling of the coronavirus, Meghan Novisky, a Cleveland State University professor who focuses on the health consequences of incarceration, told the Ohio Capital Journal. “If there are no symptoms, you can make the claim that people aren’t suffering.”
There is an obvious moral imperative for the state to provide basic protections to the people it imprisons. As many incarcerated people at Marion said in interviews, their prison sentence should not become a death sentence simply because they have no way to shield themselves from the coronavirus. But protecting the general well-being of people who live near a prison or jail is another reason to keep COVID-19 from tearing through the country’s detention facilities.
“We’ve been saying for decades, correctional health is public health,” said Dr. Brie Williams, a professor of medicine at the University of California, San Francisco who specializes in correctional health.
“Hundreds of thousands of correctional officers and correctional health care workers enter and exit these facilities every day. They return to their families, they return to their communities at the ends of their shift. They shop in the grocery stores, they seek medical care in the same health care facilities, they walk in the same parks, they send their kids on bike rides in the same areas as the rest of the community, and they bring back and forth, into and out of the jails and prisons where they work, any exposures that they’ve had during their time in the community or in the system,” Williams said.
That concern is particularly relevant in the Marion area. “We are a relatively impoverished community and a lot of people in our community work at the prisons,” said Todd Schneider, president of the Marion City Council. During one town council meeting, a member of the community compared people who work in prisons or nursing homes and wear their uniforms when they go to the grocery store to “Typhoid Mary,” said Schneider.
Health care facilities in prisons are typically designed to treat chronic conditions, like high blood pressure or diabetes, and minor injuries that require stitches. They are not generally equipped with ventilators or breathing machines to provide lifesaving respiratory support, professor Williams said. When incarcerated people become seriously ill, the plan is for them to get triaged at the on-site medical center and then transferred to a hospital in the community.
But prisons are often located in rural areas and rural areas often have smaller hospitals. “So you can just imagine the impact of an outbreak at a 2,000-person prison on a small community hospital,” Williams said.
As of July 1, 69 people incarcerated at Marion have been admitted to Wexner Medical Center, according to Smith. The highest number of prisoners in that hospital at any one time was 26, during the week of April 12. Generally, hospitals in the area do not appear to have been overwhelmed by the outbreak — but there is evidence of community spread from the prison into the surrounding community.
Even removing the more than 2,000 confirmed cases of people incarcerated at MCI from the count, Marion County has more coronavirus cases per capita than almost anywhere in the state, including the much more densely populated Cuyahoga and Franklin counties.
“What happens in our institutions is kind of reflective of what’s happening in the community,” Mabe said.
The corrections department says the prisoners at Marion are better now; the state claims that 2,042 incarcerated people who tested positive for COVID-19 have “recovered” from the virus. But most of the people who tested positive have not been retested to confirm they are now negative. Instead, people are placed in the “recovered” category based on their symptoms, even though many of those who tested positive never experienced symptoms in the first place.
“How they came to this conclusion without testing everyone again I don’t know,” White wrote in a JPay message. When White told medical staff at the prison in late May that he still had a bad cough, he was told it probably wasn’t related to the coronavirus. “They jus trying to sweep this whole thing along wit me under the rug,” he wrote.
According to Smith, people in Ohio’s prisons are considered to be recovered once they are 14 days past the onset of symptoms and free of symptoms for 72 hours. When these criteria are met, she said, the individual is referred to a physician or a nurse practitioner “who completes the recovery assessment considering the totality of the patient’s health status.” Individuals may receive a second test or antibody testing “in some instances,” but that’s a decision made on a “case-by-case basis,” Smith continued.
Relying on symptom-based assessments about COVID-19 has already proven to be a deadly mistake at a federal prison in California. Adrian Solarzano, a 54-year-old who was incarcerated at Terminal Island, died on May 24, after the Federal Bureau of Prisons had proclaimed him “recovered” from the coronavirus based on his lack of visible symptoms.
D’Augustino, Stores and Willis Williams are in the process of suing Ohio’s governor and top corrections officials on the grounds that the response to the pandemic at Marion violated Eighth Amendment prohibitions against cruel and unusual punishment. They will need to prove that the state acted with “deliberate indifference” to their medical needs. Without access to the internet, they sometimes would ask me to send copies of news reports and legal documents or to transcribe part of a press conference they had seen on TV so they could reference it in their complaint.
D’Augustino wrote the 50-page complaint by hand, without help from a lawyer. Williams proofread, keeping an eye out not only for typos but also for penmanship — you have to dot i’s hard for it to show up on a copy machine, he explained. It took weeks to get the document mailed from the prison to the federal court.
“It’s a very tedious process, and it’s pretty much set up for laymen to fail,” Williams wrote in a JPay message. “But we can’t be discouraged by that.”
The Ohio Department of Rehabilitation and Correction’s response to COVID-19 at its prison in Marion was, objectively, a failure. An overwhelming majority of the people under their care got sick, more than a dozen died, and there doesn’t appear to be an adequate plan in place to prevent another outbreak in the future.
That’s been true of the American prison system as a whole during this pandemic. State and federal prisons across the country have failed to prevent a total of more than 600 deaths since March.
Due to decades of draconian sentencing laws and a broken parole system that often fails to account for overly harsh sentences or individuals’ reform, Ohio imprisons thousands more people than its prisons were designed to hold.
“I don’t think, by and large, that the problem lies at the feet of Annette Chambers-Smith,” said David Singleton, executive director of the Ohio Justice and Policy Center. “She and her staff have tried to do as good a job as possible getting out in front and planning.”
The real problem, Singleton said, is Gov. DeWine’s failure to sign off on a large-scale reduction of the prison population. “You could do all the planning in the world and I don’t see how you prevent what’s happening at a place like Marion — and also at Pickaway — if you don’t actually substantially reduce the prison population,” Singleton said.
The numbers problem is clear to the people imprisoned inside Marion Correctional Institution, too. “The story isn’t that more than 2,000 guys came up with positive COVID-19,” White said in an interview. “My thing is: why was there more than 2,000 guys in a prison that was designed for 1,500?”
“I’m not begging to go home,” said Banks, who noted that he didn’t expect to be released even if the governor moved to depopulate the state’s prisons. “I’m begging to be safe.”
“If I have to be in prison, I want to be safe.”
Calling all HuffPost superfans!
Sign up for membership to become a founding member and help shape HuffPost’s next chapter
Credit: Source link